

Tocolytic Therapy for Improving Preterm Birth Outcome
One of the problems that has had a strong impact on perinatal morbidity and mortality worldwide is prematurity, especially when it occurs before 34 weeks of gestation. Respiratory distress syndrome, necrotizing enterocolitis, intraventricular hemorrhage and neonatal sepsis are some of the complications of prematurity.1
Great efforts in fetal medicine have been devoted to the identification of pregnant women at risk of preterm birth and its prophylaxis; however, in the setting of threatened premature labor, tocolytic drugs are useful, including calcium channel blockers, oxytocin antagonists, beta-adrenergic agonists, and non-steroidal anti-inflammatory drugs (NSAIDs). These have the ability, through several mechanisms, to stop the activity of the uterine muscle and prolong the pregnancy in order to administer antenatal corticosteroids, fetal neuroprotection with magnesium sulfate and transferring the patient to a care center that has neonatal intensive care.2
Currently, there are no United States Food & Drug Administration (FDA) approved medications for tocolysis. All medications are administered as off-label indications. However, these medications are still effective and should be used when clinically indicated.3
Tocolysis is recommended in patients with gestations <34 weeks with threatened preterm labor for a maximum of 48 hours, as long as there are no contraindications for this therapy. After this period of time, tocolytics are ineffective in preventing preterm delivery and in improving neonatal outcomes, so they are not recommended for this purpose.2
Tocolysis has also been used in the setting of external cephalic version, which may be a risk factor for the development of preterm labor; and uterine tachysystole, defined as 5 or more uterine contractions in 10 minutes.4
Citations:
1) Institute of Medicine. 2007. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: The National Academies Press.
2) American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics. Practice Bulletin No. 171: Management of Preterm Labor. Obstet Gynecol. 2016;128(4):e155-e164. doi:10.1097/AOG.0000000000001711
3) Mayer C, Apodaca-Ramos I. Tocolysis. [Updated 2022 Apr 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562212/
4) Heuser CC, Knight S, Esplin MS, Eller AG, Holmgren CM, Manuck TA, Richards D, Henry E, Jackson GM. Tachysystole in term labor: incidence, risk factors, outcomes, and effect on fetal heart tracings. Am J Obstet Gynecol. 2013 Jul;209(1):32.e1-6.
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


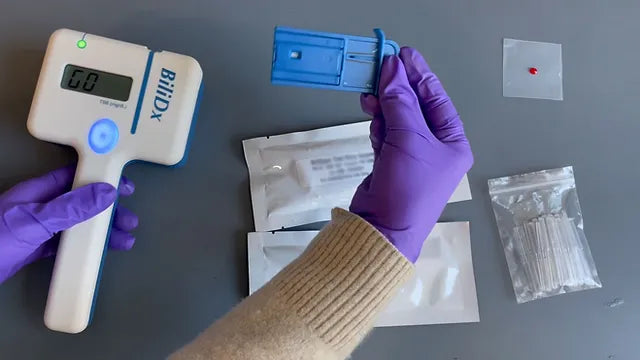
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More
Clinical Indications for Applying (and Removing) the NASG: Rule of 20
The garment must be removed upon reaching hemodynamic stability for at least two hours, where it is evident:
- Blood loss less than 50 mL/hour
- Pulse less than 100 beats per minute


{formbuilder:60191} 
