

Maternity Care Deserts in the United States
Looking Ahead: What Must be Done to Address Maternity Care Deserts
The United States faces a drastically high maternal mortality rate compared to other financially comparable developed nations. This issue is exacerbated by areas of the country where obstetric care appears to be completely absent from communities and even whole counties. March of Dimes recently uploaded their 2022 report concerning maternity care deserts in the United States. The report breaks down updated statistics on the prevalence of maternity care deserts, and evaluates them in terms of trends from previous years, reviews the effectiveness of solutions that have been implemented thus far, and offers guidance on future solutions.
March of Dimes defines maternity care deserts as “any county without a hospital or birth center offering obstetric care and without any obstetric providers.” The report details that there are 1119 counties in the United States (36% of all counties in the country), classifiable as maternity care deserts, and approximately 2.2 million women live in these regions with 146,000 babies born per year into an environment matching the classification criteria. This issue compounds further with an estimated 4.7 million women living in counties characterized as having limited access to maternity care and 300,000 babies being born into those counties (1).
Maternity care deserts are due in part to the closure of maternity services. Between 2006 and 2020, over 400 obstetric services across the country closed. As of right now, it can only be anticipated that these numbers will continue to trend upwards as more and more obstetric care units in hospitals close their doors. In 2022 alone, 11 health systems ended obstetric services in response to low birth volumes and staff shortages (2).
Unfortunately, over half of the identified maternity care deserts are in rural regions of the country, and Black, Latinx, and Native American mothers are disproportionately impacted by this lack of care in specific regions of the country, groups of the population already at higher risk for severe birthing complications and maternal mortality.
Government agencies and private entities must act quickly and effectively in order to mitigate the effects of maternity care deserts and reduce the prevalence of them over all. In order to accomplish this, several initiatives and policy recommendations are already in place.
Rural Maternity and Obstetric Management Strategies (RMOMS) Grants
In 2019, the Health Resources and Services Administration piloted the RMOMS program. The goal of this program was to provide funding to organizations wishing to implement programs to increase access to obstetric care services in rural communities. Grants run four years at a time, and positively impact communities by improving the health of women and infants. Since the start of the program, 10 initiatives in 10 different states have been implemented or are in the process of being implemented.
One project from the first cohort took place in New Mexico and was called the New Mexico Rural Obstetrics and Maternal Services (ROAMS) Network. The funding enabled the program to open two new prenatal clinics in former maternity care deserts as well as enhance telehealth services in the region to allow women to be more engaged with prenatal, and postpartum care. Telehealth kits were distributed to women with higher risk pregnancies, resulting from conditions such as diabetes or hypertension. These kits include educational content, devices to measure blood pressure and other vital signs at home that can be communicated to providers. The ROAMS project also expanded access to social services for expectant mothers via family navigators and lactation consultants.
Mobile Obstetric Care Clinics
More often than not, women living in areas designated as maternity care deserts are deprived of any opportunity to receive prenatal care to support a healthy pregnancy. Lack of prenatal care correlates with higher levels of risk for low birth weight, preterm labor, and maternal and infant mortality (3). Thus, it is crucial to increase access to prenatal care when planning to aid women in maternity care deserts.
In some states where several counties are classified as maternity care deserts, this effort has already begun via the introduction of mobile or satellite obstetric care units. In Ohio for instance, Ohio State University, in partnership with Moms2B, has introduced the Community Care Coach, a large coach bus that provides obstetric services to mothers in need in the community. Other states may benefit from implementing a service such as this one, and could even work to build upon current efforts in this manner through partnerships with community based organizations, to bridge the gap in access to maternal health services.
Future Policy and Research Avenues
While the aforementioned projects have improved outcomes for some women living in maternity care deserts, there is still much work to be done to fully address the discrepancies in maternal healthcare that exist nationwide. Because March of Dimes estimates that Medicaid covers about 50% of births in maternity care deserts, one policy recommendation that could be more widely implemented is ensuring all women have access to coverage for midwifery care and freestanding birth centers under Medicaid, regardless of the state they live in. While federal regulations currently require states to cover these services, some insurance providers have not been financing these services in accordance with the most up to date regulations (4).
Along the same lines, Medicaid programs should also cover doula services. This is because research demonstrates that mothers are subject to increased clinical benefits from continual support during labor, including reductions in rates of cesarean sections (5). Therefore, Medicaid would also realize cost savings from this policy change.
Another recent call to research as a possible solution to address the needs of expectant mothers in maternity care deserts is the use of drones to deliver needed maternal health resources. While this has not yet been tested, studies have requested future drone research in relation to healthcare delivery focus specifically on maternal health (6) in hopes of decreasing maternal mortality rates in maternity care deserts.
- https://www.marchofdimes.org/sites/default/files/2022-10/2022_Maternity_Care_Report.pdf
- https://jamanetwork.com/journals/jama-health-forum/fullarticle/2800629
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4285828/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7772638/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3617571/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7478386/
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


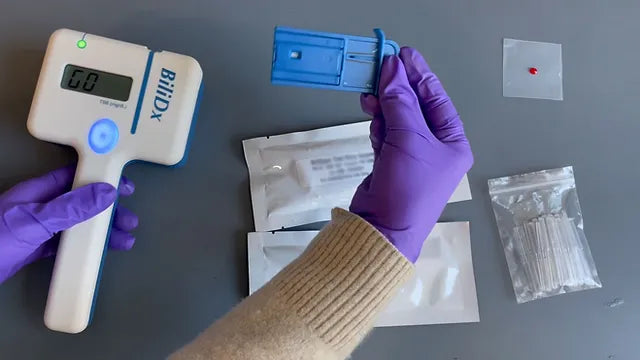
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More
Clinical Indications for Applying (and Removing) the NASG: Rule of 20
The garment must be removed upon reaching hemodynamic stability for at least two hours, where it is evident:
- Blood loss less than 50 mL/hour
- Pulse less than 100 beats per minute


{formbuilder:60191} 
