

Including pregnant women in vaccine research
Last month, the Pregnancy Research Ethics for Vaccines, Epidemics, and New Technologies (PREVENT) Working Group released a long overdue report on the issue of including pregnant women in vaccine research. The report comes after the World Health Organization’s (WHO) vaccine advisory group said it was not recommending Ebola vaccination for pregnant women or women who are lactating in the current outbreak in the Democratic Republic of Congo (DRC), when a new vaccine was delivered in the worst affected areas. The vaccine is a live vaccine, which is not normally given to pregnant women.
The safety evidence of the Ebola vaccine in pregnant women is unclear. However, what is clear is that approximately 90% of pregnant women who are infected with Ebola die from the disease and nearly 100% of pregnancies in Ebola infected women end in miscarriage or neonatal death. These numbers clearly show that preventing Ebola in pregnant women during an acute outbreak is vital when the outcomes are so severe. When the risk of mortality is so high, the benefits of offering the vaccine outweighs the risks. Denying pregnant women vaccination highlights yet again the unequal emphasis placed on the life of the woman carrying the pregnancy. In general, clinical guidelines state that the life of the mother should be prioritized over the fetus when mother and fetus are in danger. As Ebola has such a high mortality rate, simply not giving the vaccine to pregnant women because of a fear of affecting the unborn fetus, places more importance on the life of the fetus than the mother.
The problem seen in the Ebola outbreak in the DRC is not unique. Pregnant women tend to be excluded from vaccine research to protect them from risks. However, by doing so, a vicious cycle is created whereby pregnant women are excluded from studies meaning evidence cannot be generated, which further excludes them from vaccinations during outbreaks. The fear of adverse effects towards the fetus and mother is sometimes not based on evidence and this can create more harm.
The PREVENT group has brought together experts in the ethics, obstetrics, pediatrics, public health and vaccine research field to help tackle this evidence gap. Their report includes 22 recommendations which are centered around the importance of offering vaccines to pregnant women during epidemics (this should be the default), the inclusion of pregnancy status in real world studies (for e.g. it is likely that during the Ebola outbreak, pregnancy status would not have been determined in women who were obviously not pregnant at the time of vaccination. Therefore, there would have been women who were pregnant who received the vaccine and were not followed up), assessment of risks and benefits, the expert opinion of maternal fetal experts in the inclusion and exclusion of pregnant women in studies, and the perspectives of pregnant women themselves to guide vaccine research.
There is a positive shift to include pregnant women in clinical trials, but the progress is slow. Research and academic communities are only just realizing the importance of disaggregating data by sex and including women in clinical trials – finally acknowledging that conditions and drugs affect women differently to men. Hopefully, this new report will push the research community towards creating an evidence base for those who are pregnant and for women as a whole.
Photo credit: NIH
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


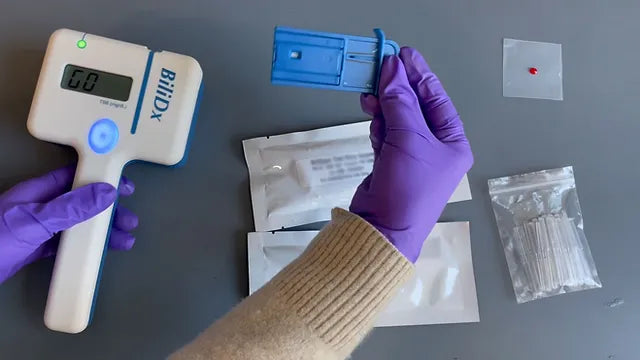
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More
Clinical Indications for Applying (and Removing) the NASG: Rule of 20
The garment must be removed upon reaching hemodynamic stability for at least two hours, where it is evident:
- Blood loss less than 50 mL/hour
- Pulse less than 100 beats per minute


{formbuilder:60191} 
