

Global maternal health: It's going to get a lot more complex
Maternal health is changing dramatically.
Global maternal health has been focused on ending maternal mortality in the developing regions of the world, and rightly so as they are so preventable. We are tackling the problem by targeting the direct causes of maternal deaths (deaths resulting from obstetric complications of pregnancy) such as PPH, preeclampsia or sepsis. However, what we are seeing now in many parts of the world is the ‘obstetric transition’ – a shift from mainly direct causes of maternal death to indirect causes of maternal death (death caused by existing disease, or disease that developed during pregnancy, but not due to the pregnancy itself).
Non-communicable diseases (NCDs) now account for approximately 65 percent of deaths occur in women. They also contribute to indirect maternal deaths, making up one-third of all maternal deaths. NCDs in pregnancy include cardiac disease (including hypertension), endocrine disease, metabolic conditions such as diabetes, anemia, respiratory disease, cancer, and mental health conditions. Other causes of indirect deaths include HIV and malaria, and 15% of maternal deaths are due to pre-existing conditions. We have seen a decline in direct maternal deaths, which can be attributed to improved emergency obstetrical care. However, indirect deaths are rising and have largely been ignored.
Lack of attention to indirect deaths stems from measurement difficulties. Disaggregating maternal death data by indirect and direct causes is difficult in developing countries as detailed patient records are limited. However, countries without abundant resources such as South Africa have shown that organizing a system that investigates into maternal deaths is a possibility. It has managed to reveal deaths from indirect causes, highlighting that it is an issue that desperately needs addressing by the government.
Even if data is available, rising indirect deaths and the increasing prevalence of NCDs only adds to the complexity of delivering maternal healthcare. These deaths and conditions cannot be managed by emergency obstetrical care, but require organized health systems that are able to monitor and manage these women at preconception, antenatally, during labor and postnatally. Women that suffer from pre-existing conditions require medical specialists during pregnancy, as well as an obstetrician, and so vertical healthcare programs will no longer cut it. A life course approach has been suggested whereby women are cared for across their lifespan, to seize opportunities to prevent disease earlier on in life. NCDs are the result of the interaction between genetics and the external environment, which means there is ample opportunity to prevent, detect, or manage these conditions prior to pregnancy. However, a life course approach is going to require strong primary, secondary and tertiary care, posing a significant problem for low/middle income countries or fragile states that are still trying to ensure they have basic emergency care in place.
Maternal healthcare now more than ever requires actual health systems. However, barriers to healthcare access still persist. Societal norms, poor income, far distances from health centers, and the systemic undervaluing of women make this a much more complex issue, and will make a life course approach difficult to achieve. There is a need to look beyond the fact that healthcare for women is just about maternal and reproductive care. They are also affected by disease and disability separate from pregnancy, just like everyone else.
By Shreya Patel
Photo credit:
Sophia Paris, 2010
Doctor Examines Haitian Woman Living in Port-au-Prince Stadium
A doctor examines a pregnant Haitian woman living in a tent inside Port-au-Prince's National Stadium.
03 February 2010
Port-au-Prince, Haiti
Photo # 426985
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


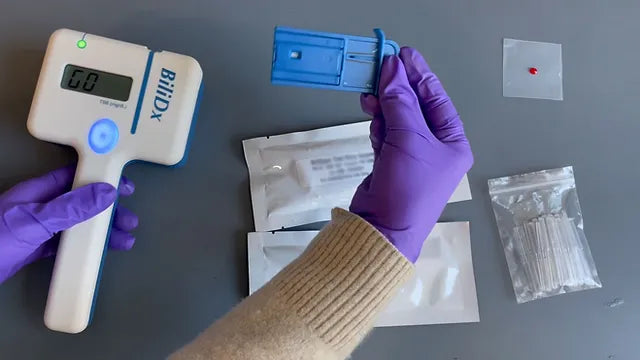
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More
Clinical Indications for Applying (and Removing) the NASG: Rule of 20
The garment must be removed upon reaching hemodynamic stability for at least two hours, where it is evident:
- Blood loss less than 50 mL/hour
- Pulse less than 100 beats per minute


{formbuilder:60191} 
