

Bringing Hope to the Democratic Republic of Congo with Channel Initiative
At Maternova, we consider ourselves incredibly lucky to have partners located around the world. Its these fearless entrepreneurs and philanthropists who make what we do so worthwhile, and in some cases possible. One of our favorite groups is Channel Initiative. Founded by Dominique Vidale-Plaza, they are shaking things up in the DRC and empowering women and children with sustainable healthcare. Not only is this incredibly brave, its desperately needed. Many medical clinics are days apart for foot travelers.
We wanted to see if our friends at Channel Initiative had an update for us on how they are progressing. This will be a two part series with todays entry covering both the needs of this vulnerable population along with some of the lessons Dominique and team have learned along the way. Enjoy!
Part 2 -- Lessons Learned and Moving forward
Lessons don’t ever stop in the Democratic Republic of Congo, and in most countries like it. They’re every day and sometimes every hour. Continuing to work with Panzi Hospital and Channel Initiative has brought many, many other opportunities for lessons and for coming to a place of deeper understanding on the complex needs of women and girls in the rural and under-served areas of the Democratic Republic of Congo.
It is obvious that there is a glaring need for health services in communities like these, that can ensure care to women and girls when they need it the most, when they are giving birth, when they have experienced sexual violence or when their children are ill. These services cannot only cater to the physical, they also need to respond the holistic needs of the clients who present, the psychological and emotional needs in particular, that so often go neglected. These services, whether they come via facilities, skilled providers, or community health advocates, are the frontline in communities like these, in the fight against maternal mortality, and the fight against sexual violence and its impact as well. Rural service providers are first-responders, yet, they are under-resourced, their opinion and input in provincial and national policy development is largely ignored, and they are unable to do their jobs to the best of their abilities. They need to be equipped, resourced, bolstered, encouraged and supported.
Likewise, women and girls themselves need to be empowered and encouraged to seek these services themselves. There is a wide range of socio-economic factors that prevent, hinder or discourage women from seeking care when they need to. These include the prohibitive cost of health-care, poor transport and/or road infrastructure, myths and misunderstandings about different health services, especially reproductive and/or gynecological health services, lack of knowledge and fear of stigmatization in cases of fistula, prolapse or sexual violence. I can’t tell you how many women I’ve met, who have hid STDs, being raped, or miscarriages for several years from their families, even if they were in crippling pain, just so as not to have to deal with shame, stigma, whispers, or staring eyes. Likewise, I can’t tell you how many times, we have had to correct almost funny misconceptions about contraception, sex, menstruation and more. The education, involvement and empowerment of women and girls in rural Democratic Republic of Congo need to be as much parts of health-programming in these communities as does, a focus on health service providers. It goes both ways, far beyond just the availability of health services, and into ensuring that there is a demanding, empowered and informed population.
These are just brief explanations of two key lessons I have learned in the last few years – equipping, empowering and involving, both the frontline service providers, and the women and girls in need of the services. It might seem simple and obvious, but these two elements (particularly, the involving of their input and opinions) are sorely missing from health programs in the DRC in particular, and to their detriment. Programs that ignore the frontline, that ignore equipping, educating and empowering the female populace so that they will demand services on their own, organizations that ignore ensuring that the frontline service providers can go on responding to this demand, long after they have pulled out, can never achieve the impact that they’re setting out to achieve. I’m thrilled that we get to work with Maternova on these two components, and in fulfilling our mission of ensuring that women in under-reached and under-served communities have access to care that treats, restores and empowers them.
We wanted to see if our friends at Channel Initiative had an update for us on how they are progressing. This will be a two part series with todays entry covering both the needs of this vulnerable population along with some of the lessons Dominique and team have learned along the way. Enjoy!
Part 2 -- Lessons Learned and Moving forward
Lessons don’t ever stop in the Democratic Republic of Congo, and in most countries like it. They’re every day and sometimes every hour. Continuing to work with Panzi Hospital and Channel Initiative has brought many, many other opportunities for lessons and for coming to a place of deeper understanding on the complex needs of women and girls in the rural and under-served areas of the Democratic Republic of Congo.
It is obvious that there is a glaring need for health services in communities like these, that can ensure care to women and girls when they need it the most, when they are giving birth, when they have experienced sexual violence or when their children are ill. These services cannot only cater to the physical, they also need to respond the holistic needs of the clients who present, the psychological and emotional needs in particular, that so often go neglected. These services, whether they come via facilities, skilled providers, or community health advocates, are the frontline in communities like these, in the fight against maternal mortality, and the fight against sexual violence and its impact as well. Rural service providers are first-responders, yet, they are under-resourced, their opinion and input in provincial and national policy development is largely ignored, and they are unable to do their jobs to the best of their abilities. They need to be equipped, resourced, bolstered, encouraged and supported.
Likewise, women and girls themselves need to be empowered and encouraged to seek these services themselves. There is a wide range of socio-economic factors that prevent, hinder or discourage women from seeking care when they need to. These include the prohibitive cost of health-care, poor transport and/or road infrastructure, myths and misunderstandings about different health services, especially reproductive and/or gynecological health services, lack of knowledge and fear of stigmatization in cases of fistula, prolapse or sexual violence. I can’t tell you how many women I’ve met, who have hid STDs, being raped, or miscarriages for several years from their families, even if they were in crippling pain, just so as not to have to deal with shame, stigma, whispers, or staring eyes. Likewise, I can’t tell you how many times, we have had to correct almost funny misconceptions about contraception, sex, menstruation and more. The education, involvement and empowerment of women and girls in rural Democratic Republic of Congo need to be as much parts of health-programming in these communities as does, a focus on health service providers. It goes both ways, far beyond just the availability of health services, and into ensuring that there is a demanding, empowered and informed population.
These are just brief explanations of two key lessons I have learned in the last few years – equipping, empowering and involving, both the frontline service providers, and the women and girls in need of the services. It might seem simple and obvious, but these two elements (particularly, the involving of their input and opinions) are sorely missing from health programs in the DRC in particular, and to their detriment. Programs that ignore the frontline, that ignore equipping, educating and empowering the female populace so that they will demand services on their own, organizations that ignore ensuring that the frontline service providers can go on responding to this demand, long after they have pulled out, can never achieve the impact that they’re setting out to achieve. I’m thrilled that we get to work with Maternova on these two components, and in fulfilling our mission of ensuring that women in under-reached and under-served communities have access to care that treats, restores and empowers them.
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


What's new in menstrual health management: an interview with the Founder of Asan
The Asan cup is a patented menstrual cup with a unique removal ring, which makes it the easiest cup to insert and take out. The bell-shaped design ensures that the cup sits comfortably, and the red colour of the cup prevents it from staining over time.
Read More

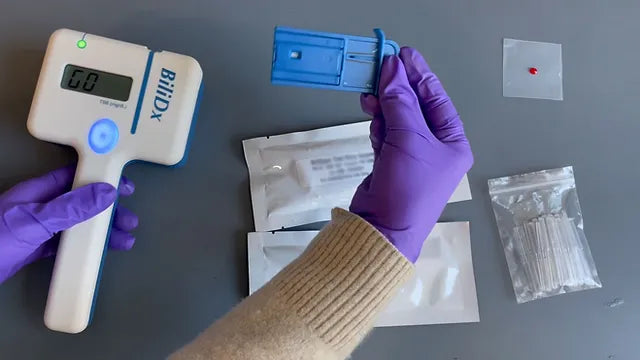
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More

{formbuilder:60191} 
