

Are multiple micronutrient supplements superior to the traditional iron-folic acid supplements taken during pregnancy?
It is common in low- and middle-income countries for women to experience micronutrient deficiencies as a result of poor diet. This becomes a particularly acute issue in pregnancy due to an increase in the nutrient requirements of both mother and fetus. Deficiencies in micronutrients like vitamin A, iron, iodine, and folate can negatively impact the health of both the mother and fetus.
To address this issue, in 1999, UNICEF, United Nations University and the World Health Organization (WHO) came together and agreed on the composition for a multiple micronutrient tablet that included vitamins A-E, niacin, folic acid, copper, selenium, iodine, iron and zinc.
However, the only treatment for micronutrient deficiencies in pregnant women fully endorsed by WHO currently is iron and folic acid (IFA) supplementation, leaving out many other important micronutrients that can impact maternal and fetal health. In their most recent publication on this topic, a 2016 publication on antenatal care, WHO stated that current evidence on multiple micronutrient supplementation (MMS) shows that it may reduce the risk of poor birth outcomes like low birth weight (LBW) and small size for gestational age compared with IFA alone, but that there is also evidence of risk and gaps in evidence. Although WHO acknowledged that the advantages of MMS might outweigh the disadvantages in populations with a high prevalence of nutritional deficiencies, overall the disadvantages propelled WHO away from a recommendation.
Recent reviews however are affirming the potential effectiveness of MMS over IFA alone during pregnancy in birth outcomes and infant survival. A Cochrane review published in 2019 that looked at 21 trials found that pregnant women who received MMS had fewer low birth weight babies, fewer babies born at a small size for their gestational age, and fewer preterm births, compared to pregnant women who received iron (with or without folic acid) or a placebo. The review concluded that the findings could provide “a basis to guide the replacement of iron and folic acid supplements with multiple‐micronutrient supplements for pregnant women in low‐ and middle‐income countries.”
A similar review published inThe Lancet Global Healthin 2017, found the same reductions. In reviewing 17 randomized trials, they found a 12-14% reduction in low birthweight, a 7-8% reduction in preterm delivery, and a 3-6% reduction in small size for gestational age. In addition, the review found that MMS had a larger effect on birth outcomes among women with either anemia or low BMI at the start of trials. While MMS had no overall effect on mortality of an infant at any point during the first year of life,among female infantsit significantly reduced the risk of early neonatal, neonatal, 6-month, and infant mortality. MMS also reduced the risk of 6-month mortality in infants born to women who were anemic at the beginning of the trials. This data was applied in a study published in theAnnals of the New York Academy of Sciences last year that modeled the effects of switching from IFA to MMS in Bangladesh and Burkina Faso. Using the current coverage levels of the IFA program in the two countries, the study found that by shifting from IFA to MMS it was predicted that 7,500 infant lives would be saved and 15,000 preterm births avoided in Bangladesh over the course of one year. In Burkina Faso, it was predicted that 484 infant lives would be saved and 550 preterm births avoided.
The costs associated with shifting from IFA to MMS for pregnant women are significant. MMS is approximately 35% more expensive than IFA tablets. However, the consensus of these reviews, as well as the model, in showing the positive impact of MMS compared to IFA in birth outcomes and infant survival suggest that it may be time for Ministries of Health and global health organizations to start considering (if they haven’t already) switching to MMS for pregnant women in order to continue improving and saving the lives of infants around the globe.
By Mikaela Carrillo
References
(1)WHO Recommendations: Multiple micronutrient supplementation during pregnancy
(2)WHO recommendations on antenatal care for a positive pregnancy experience
(3)Multiple‐micronutrient supplementation for women during pregnancy,Cochrane Library, 2019
(4)Modifiers of the effect of maternal multiple micronutrient supplementation on stillbirth, birth outcomes, and infant mortality: a meta-analysis of individual patient data from 17 randomised trials in low-income and middle-income countries,The Lancet Global Health, 2017
(5)Replacing iron‐folic acid with multiple micronutrient supplements among pregnant women in Bangladesh and Burkina Faso: costs, impacts, and cost‐effectiveness,Annals of the New York Academy of Sciences, 2019
Photo Credit
Maternova
Leave a comment
Comments will be approved before showing up.
Also in The Maternova Blog


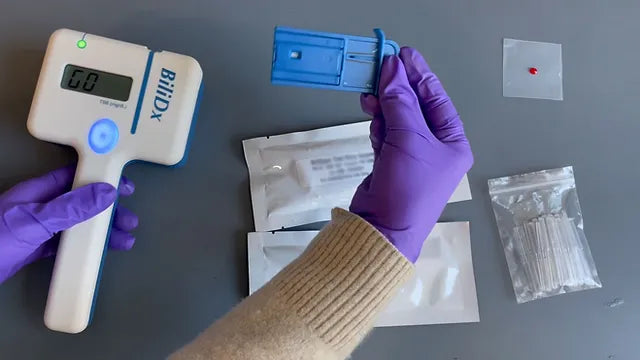
A Point of Care Bilirubinometer Using Blood: BiliDx
The BiliDx is a novel system for diagnosing jaundice. The device uniquely meets the Target Product Profile (TPP) developed as part of the NEST 360 initiative in that it allows blood-based testing at the bedside. This initiative is part of an emerging global consensus in the Every Newborn Action Plan that countries need functional WHO level-2 inpatient units to care for "small and sick newborns."
Read More
Clinical Indications for Applying (and Removing) the NASG: Rule of 20
The garment must be removed upon reaching hemodynamic stability for at least two hours, where it is evident:
- Blood loss less than 50 mL/hour
- Pulse less than 100 beats per minute


{formbuilder:60191} 
